For many, the term “OCD” has become a casual label — people say they’re “so OCD” because they like things neat or in order. But for those truly living with Obsessive-Compulsive Disorder, this phrase hits differently. OCD isn’t about being tidy or picky; it’s about living with persistent, intrusive thoughts and a relentless drive to neutralize them through compulsive behaviors.
In this article, we’ll unpack OCD the facts — not the stereotypes or social media soundbites, but the real inner experience of what it means to live with OCD.
OCD: What It Really Is?
OCD, or Obsessive-Compulsive Disorder, is a mental health condition characterized by two key components: obsessions (unwanted, intrusive thoughts, images, or urges) and compulsions (repetitive behaviors or mental actions done to relieve anxiety or prevent a feared event).
According to OCD the facts outlined by mental health professionals, it is not a personality quirk or a preference for cleanliness. It’s a chronic disorder rooted in the brain’s anxiety and control circuits, where fear and uncertainty become magnified beyond reason.
A few realities about OCD in women include:
- It’s often driven by fear, guilt, or uncertainty, not perfectionism.
- Compulsions can be physical (like checking or washing) or mental (like counting or silent reassurance).
- People with OCD recognize their thoughts are excessive or irrational but feel powerless to ignore them.
This constant mental tug-of-war between logic and fear creates immense distress and fatigue.
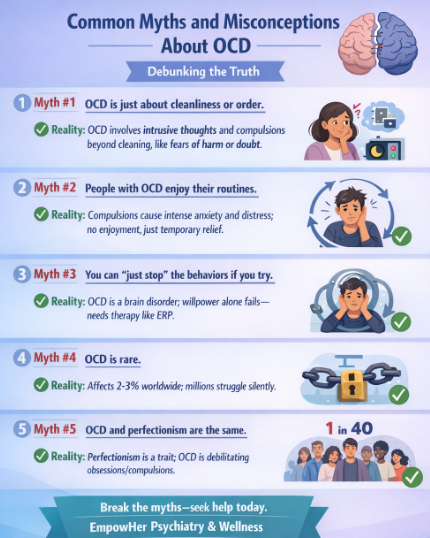
Common Myths and Misconceptions About OCD
One major reason people struggle to get help is because OCD the facts are often distorted or trivialized. Let’s clear up a few of the most damaging myths:
- Myth #1: OCD is just about cleanliness or order.
Reality: While some people have contamination-related fears, OCD can center around countless themes — morality, health, relationships, harm, religion, or even existential fears. - Myth #2: People with OCD enjoy their routines.
Reality: Compulsions are not comforting habits; they’re rituals performed out of fear, not choice. Skipping them can cause intense anxiety or panic. - Myth #3: You can “just stop” the behaviors if you try.
Reality: Knowing a compulsion doesn’t make sense doesn’t make it easier to stop. OCD operates through powerful anxiety loops that feel uncontrollable without proper treatment. - Myth #4: OCD is rare.
Reality: Research shows OCD affects millions worldwide — across genders, ages, and backgrounds. It often begins in childhood or adolescence but can also appear in adulthood. - Myth #5: OCD and perfectionism are the same.
Reality: Perfectionism is a personality trait; OCD is a disorder involving irrational fears and repetitive efforts to reduce them. They can overlap, but they’re not interchangeable.
When we separate myth from truth, OCD the facts become more empowering — opening the door for understanding, compassion, and proper treatment.
The Inner Experience: What OCD Feels Like
Living with OCD can feel like being trapped in a mental loop. You know logically that the fear may be exaggerated, but the anxiety screams louder than reason.
Here’s how that cycle often looks:
- Trigger. A thought, image, or doubt sparks discomfort. (“What if I left the stove on?”)
- Obsession. The thought grows stronger, replaying endlessly.
- Compulsion. You perform an action (checking, counting, praying) to relieve the anxiety.
- Relief. The distress briefly drops — but the brain learns that compulsions “work,” reinforcing the cycle.
Over time, this loop consumes mental energy and can severely disrupt daily life. Understanding OCD the facts through this lens helps people see why it’s not something someone can “snap out of.” It’s a neurological feedback loop that needs retraining, not reprimand.
OCD Comes in Many Forms (Not Just Cleanliness)
OCD isn’t one-size-fits-all. There are multiple subtypes, though they often overlap:
- Contamination OCD: Fear of germs, illness, or impurity leading to excessive washing or avoidance.
- Checking OCD: Repeatedly verifying doors, appliances, or tasks to prevent harm.
- Harm OCD: Intrusive fears of hurting others, even though the person has no desire to do so.
- Relationship OCD: Constant doubts about romantic relationships or feelings.
- Moral/Religious OCD (Scrupulosity): Obsessions about sin, morality, or being “bad.”
- Existential OCD: Obsessions about life, death, or the meaning of existence.
These forms can shift over time. The content of obsessions doesn’t define the disorder — the relationship to the thought does. In every case, the anxiety is irrational but feels acutely real to the person experiencing it.

Why OCD Is So Misunderstood
OCD’s invisibility makes it easy to misjudge. Many people hide their symptoms out of shame, fear of judgment, or misunderstanding. Others “mask” their compulsions by performing them mentally or privately.
Another reason OCD is misunderstood is its diverse expression — two individuals might both have OCD but with vastly different thought patterns. There’s also cultural influence: for some, religious fears dominate; for others, contamination or safety fears take center stage.
When families know OCD the facts, it becomes easier to see symptoms for what they are — not stubborn habits or overreactions, but deeply rooted anxiety loops that can be treated effectively.
The Science Behind OCD
At its core, OCD is a problem of communication between parts of the brain responsible for threat detection, habit formation, and regulation. Studies show differences in the orbitofrontal cortex, amygdala, and basal ganglia — areas that influence response to danger and repetitive thinking.
In simple terms, the OCD brain sends false alarms. It over-interprets uncertainty as threat, triggering obsessive “what if” loops. Compulsions momentarily silence the alarm, but they also teach the brain to fire it again — creating a vicious cycle of reassurance seeking and anxiety.
While we still don’t know all the answers, understanding OCD the facts in biological terms helps reduce stigma: it’s not a character flaw but a neurological condition with established treatment options.
How OCD Affects Families and Relationships

OCD doesn’t exist in isolation — it affects everyone around the person living with it. Family members often become part of the compulsions without realizing it. For example, someone might ask a loved one for constant reassurance: “Are you sure I didn’t offend you?” or “Did I lock the door?”
Over time, this dynamic can create tension or frustration. But responding from a place of compassion makes a big difference: instead of offering reassurance (which fuels the cycle), loved ones can encourage coping strategies or remind the person to use their therapy tools.
Educating families about OCD the facts transforms relationships from reactive to supportive — empowering both sides to handle episodes with understanding rather than judgment.
Recovery Is Possible: Evidence-Based Treatments
One of the most hopeful truths about OCD the facts is that recovery is absolutely achievable. While there’s no “quick fix,” evidence-based treatments can dramatically improve quality of life.
The gold-standard therapy is Exposure and Response Prevention (ERP) — a form of Cognitive Behavioral Therapy (CBT) where individuals confront their fears without performing compulsions. Over time, the brain learns that the feared outcome doesn’t occur, and the anxiety gradually weakens.
Other treatment options include:
- Medication (SSRIs) to balance serotonin and reduce obsessive loops.
- Mindfulness-based therapy to lessen rumination.
- Support groups for sharing strategies and reducing isolation.
- Lifestyle management — sleep, exercise, and diet improvements that stabilize mood and resilience.
For families, therapy can also involve education sessions — learning how to avoid reinforcing compulsions while still providing emotional safety.
Practical Coping Tools at Home
While professional support is key, daily coping techniques can help manage symptoms between sessions. Try to:
- Practice grounding techniques (deep breathing, sensory awareness).
- Keep a “mental distance” from intrusive thoughts — label them as “just thoughts.”
- Schedule intentional rest and hobbies that engage your focus without anxiety triggers.
- Use journaling to track obsessions and identify improvement patterns.
- Reward yourself for small victories, not only finished outcomes.
Healing from OCD isn’t about eliminating all intrusive thoughts — it’s about regaining control over your reactions to them.
When to Seek Professional Help

It can be hard to know when “typical stress” crosses into disorder territory. You should consider professional help if:
- Obsessions take up more than an hour a day.
- Rituals or checking behaviors interfere with work or relationships.
- You feel ruled by anxiety or guilt.
- Avoidance of triggers limits your everyday functioning.
Therapy doesn’t mean you’ve failed; it means you’re investing in a healthier, freer relationship with your thoughts.
Final Thoughts: Understanding Brings Freedom
The road to recovery starts with awareness. When people learn the facts about OCD, shame begins to lift, understanding deepens, and self-blame slowly fades. You’re not “crazy,” “lazy,” or “controlling”—you’re dealing with a genuine medical condition that can improve with patience, support, and the right tools.
If you or a loved one struggles with OCD, remind yourself of this truth: you’re not alone, and you’re not broken. The brain is remarkable—it can be retrained, soothed, and rewired. At EmpowHer Psychiatry and Wellness, we offer compassionate, women-centered psychiatric care designed to support you through OCD and related challenges. Through personalized treatment plans, therapy, medication management, and telehealth services, we walk beside you as you reclaim peace, clarity, and confidence—one step at a time.
